A Faster Way to Stop Bleeding: Saving Lives During Emergency Bleeding Through Click Clotting
Posted 3 months ago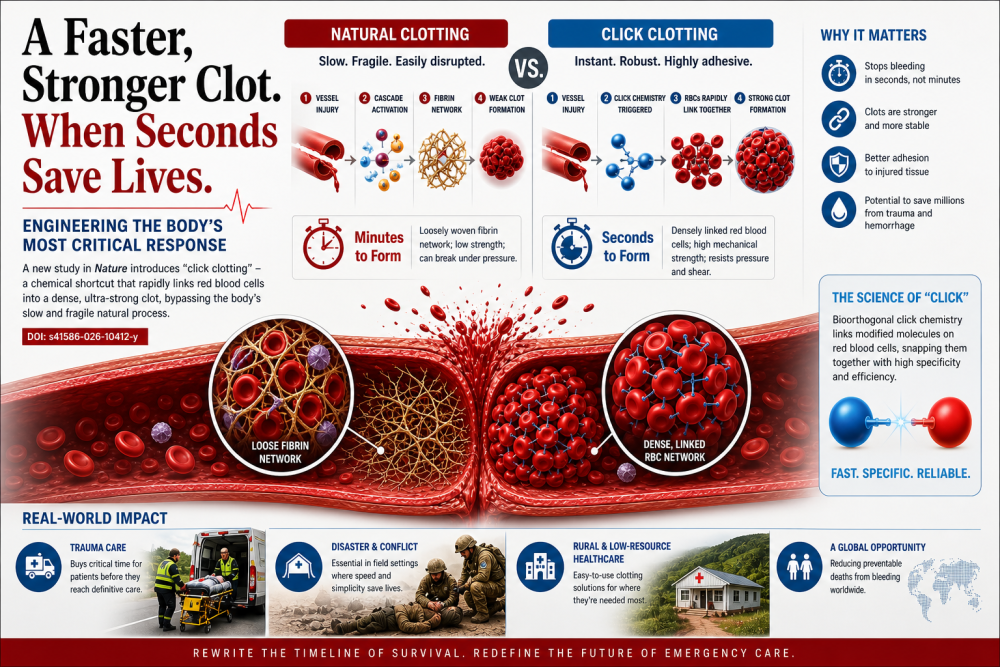
22/2026
Every second saved during bleeding can mean the difference between life and death. Acting quickly to stop bleeding gives a person a real chance to survive. When we stop the bleed in time, we’re not just saving minutes, we’re saving lives.
The human body has an extraordinary ability to heal itself, but it does so on its own timeline. When a blood vessel ruptures, a complex cascade of molecular signals is triggered, recruiting platelets and weaving protein strands into a clot that seals the wound. It is a process honed by evolution, reliable under ordinary circumstances, and quietly miraculous. Yet in moments of severe trauma, that same system can prove dangerously slow and structurally fragile.
A recent study in Nature Journal examines this biological bottleneck. It reaches a striking conclusion: the natural mechanics of blood clotting, while effective, may not be optimized for the speed and mechanical strength required in acute emergencies. The researchers approach the problem not by enhancing the existing pathway but by sidestepping it altogether.
Their method, termed “click clotting,” draws on a well-established principle in chemistry known as click reactions, highly efficient processes that rapidly and selectively join molecules. In this case, red blood cells are chemically modified to bind to one another almost instantly when triggered. Rather than waiting for fibrin networks to form gradually, the system creates a dense, interconnected cellular scaffold within seconds.
The distinction is more than technical. Conventional clots rely on a fibrin meshwork that traps blood cells in a relatively loose structure. These clots are effective under low stress but can break apart under high pressure or rapid blood flow. By contrast, the engineered clots described in this study exhibit markedly higher mechanical integrity. They adhere more strongly to damaged tissue and resist deformation, suggesting a level of robustness that natural clots rarely achieve.
From a biomedical perspective, the implications are significant. Hemorrhage remains a leading cause of preventable death, particularly in trauma settings where rapid blood loss overwhelms the body’s ability to respond. Current interventions, such as compression, surgical repair, and transfusion, are often constrained by time and accessibility. A system that can induce instantaneous clot formation could effectively shift the critical window for intervention, stabilizing patients long enough for definitive care.
At the same time, the research highlights the delicate balance inherent in hemostasis. Blood clotting is not simply a matter of forming plugs; it is a tightly regulated equilibrium between coagulation and dissolution. Disrupting this balance carries well-known risks. Excessive or misplaced clot formation can lead to thrombosis, obstructing blood flow in vital organs. Any technology that accelerates clotting must therefore contend with the challenge of precision—ensuring that clots form only where and when needed.
The study’s approach reflects a broader trend in modern medicine: the shift from biomimicry to bioengineering. Rather than replicating natural processes, researchers increasingly design systems that outperform them in specific conditions. This shift is evident across fields, from synthetic vaccines to engineered tissues to the fundamental mechanics of blood.
Importantly, the simplicity of the underlying chemistry may facilitate translation. Click reactions are already widely used in pharmaceutical and materials science applications for their reliability and specificity. Leveraging this chemistry in a clinical context could streamline development, although substantial work remains to assess safety, dosing, and long-term effects in living systems.
For global health, the potential applications are especially compelling. In regions with limited access to advanced trauma care, a fast-acting, easily deployable clotting agent could serve as a critical first line of defense. It could be used in ambulances, rural clinics, or even in the field, reducing mortality in situations where delays are unavoidable.
Still, the path forward will require careful evaluation. Preclinical success does not always translate into clinical efficacy, and the risks of altering a fundamental physiological process are nontrivial. Researchers will need to demonstrate not only that these engineered clots are effective but also that they can be controlled with high specificity.
What this work ultimately underscores is a subtle but important point: evolution optimizes for survival across populations and timescales, not for the immediacy of modern medical crises. In the gap between “good enough” and “clinically ideal,” there is room for innovation. The challenge is to ensure that, as we improve upon nature, we do not lose sight of the intricate balance that makes it work in the first place.